What Should You Pay Attention to After Rhinoplasty?
Introduction
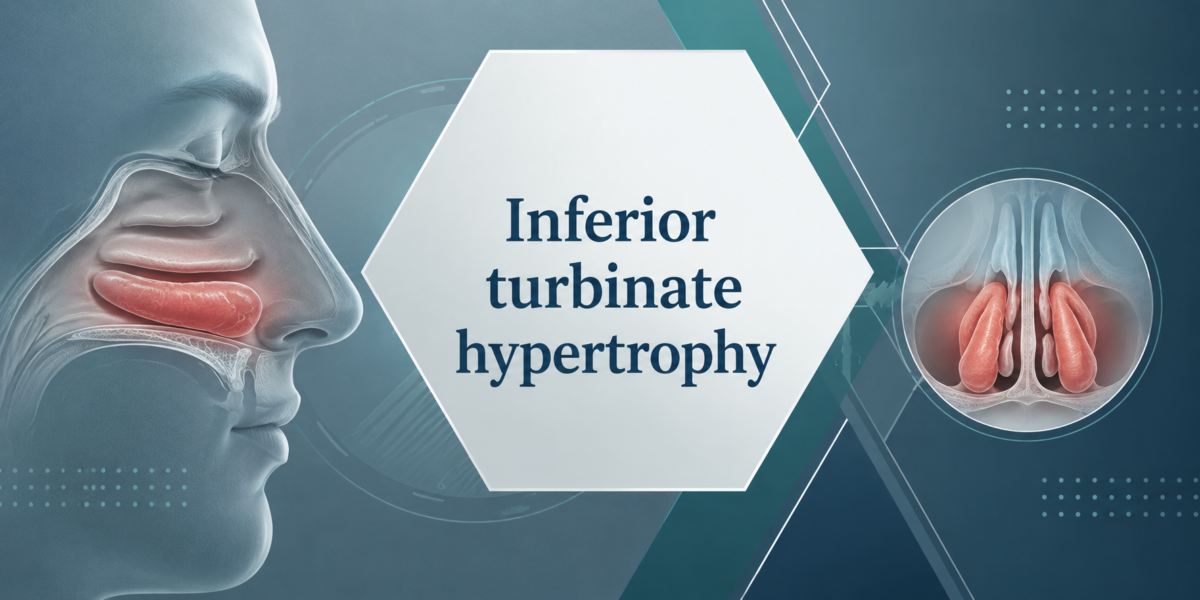
Inferior turbinate hypertrophy is one of the most common causes of chronic nasal obstruction encountered in otolaryngology practice. The inferior turbinates are highly vascular structures located along the lateral nasal wall and play essential roles in humidification, filtration, warming, and regulation of inspired air. Physiological enlargement and shrinkage of these structures occur naturally through the nasal cycle. However, persistent enlargement resulting from chronic inflammation, allergic rhinitis, vasomotor rhinitis, compensatory hypertrophy secondary to septal deviation, or environmental irritants may lead to significant nasal airway compromise. Chronic nasal obstruction caused by turbinate hypertrophy affects millions of individuals worldwide and has become an increasingly recognized public health concern because of its substantial impact on sleep quality, daytime performance, and overall wellbeing.
From a pathophysiological perspective, turbinate hypertrophy may involve mucosal edema, submucosal glandular proliferation, vascular engorgement, and in some patients, osseous enlargement of the turbinate framework. While medical therapy remains the initial treatment strategy, a considerable proportion of patients fail to achieve adequate symptom control and eventually require surgical intervention. Contemporary surgical techniques aim to improve nasal airflow while preserving the physiological functions of the turbinate mucosa. Preservation of mucosal integrity has become a fundamental principle in modern nasal surgery because excessive tissue removal may result in debilitating complications such as dryness, crusting, and empty nose syndrome.
Clinical Presentation and Diagnostic Evaluation
Patients with inferior turbinate hypertrophy most commonly present with persistent nasal obstruction, mouth breathing, snoring, facial pressure, postnasal drainage, and reduced exercise tolerance. Many individuals also report chronic fatigue, morning headaches, dry mouth upon awakening, and impaired concentration during daytime activities. Nasal obstruction may fluctuate in severity but frequently becomes persistent in advanced cases. In patients with concomitant allergic disease, symptoms such as sneezing, itching, and rhinorrhea often coexist and further exacerbate airway compromise. These symptoms may persist for years before appropriate diagnosis and treatment are established.
Comprehensive diagnostic evaluation begins with a detailed medical history and thorough physical examination. Nasal endoscopy represents the gold standard for direct visualization of turbinate size, mucosal condition, associated septal deviation, and concomitant sinonasal pathology. Endoscopic examination allows differentiation between mucosal hypertrophy and structural abnormalities requiring simultaneous correction. Additional diagnostic tools such as acoustic rhinometry and rhinomanometry may provide objective assessment of nasal airway resistance and treatment outcomes. Computed tomography imaging is particularly valuable in selected patients with chronic rhinosinusitis, severe septal deformities, or suspicion of anatomical variations contributing to nasal obstruction.
An important consideration during evaluation is the identification of underlying etiological factors. Allergic rhinitis remains one of the most frequent causes of turbinate enlargement worldwide. Environmental pollutants, smoking exposure, chronic sinus inflammation, hormonal influences, medication induced rhinitis, and compensatory hypertrophy secondary to septal deviation may also contribute significantly to disease progression. Successful long term management requires not only correction of the enlarged turbinate tissue but also treatment of these underlying pathological processes.
Impact on Sleep and Quality of Life
The influence of chronic nasal obstruction on sleep quality and overall quality of life has gained increasing scientific attention during recent decades. Nasal breathing plays a fundamental role in maintaining normal sleep physiology. Persistent obstruction resulting from inferior turbinate hypertrophy increases upper airway resistance, promotes mouth breathing, and may contribute to snoring as well as sleep disordered breathing. Several clinical studies have demonstrated significant associations between chronic nasal obstruction and poor sleep efficiency, frequent nocturnal awakenings, excessive daytime sleepiness, and diminished cognitive performance.
Patients suffering from chronic turbinate hypertrophy frequently describe profound deterioration in daily functioning. Reduced sleep quality often leads to persistent fatigue, irritability, decreased work productivity, impaired academic performance, and reduced participation in social activities. Many individuals experience difficulty concentrating and report memory disturbances that negatively affect professional and personal life. Furthermore, chronic mouth breathing may predispose patients to recurrent pharyngitis, xerostomia, and worsening of existing respiratory disorders. Consequently, timely diagnosis and appropriate treatment of turbinate hypertrophy are essential not only for restoration of nasal airflow but also for substantial improvement in overall health related quality of life.
The relationship between nasal obstruction and obstructive sleep apnea deserves particular attention. Although turbinate hypertrophy alone may not directly cause obstructive sleep apnea, it significantly increases upper airway resistance and may aggravate preexisting sleep disordered breathing. Improvement of nasal patency following surgical treatment has been shown to enhance patient comfort, improve tolerance to continuous positive airway pressure therapy, and reduce subjective sleep related complaints. Therefore, comprehensive evaluation of sleep symptoms should constitute an integral component of the assessment process in patients with chronic nasal obstruction.
Medical Management
Initial treatment of inferior turbinate hypertrophy generally involves conservative medical therapy. Intranasal corticosteroid sprays remain the cornerstone of treatment because they effectively reduce mucosal inflammation and edema. Antihistamines, leukotriene receptor antagonists, saline irrigations, and allergen avoidance strategies may provide additional symptomatic relief in selected patients. Immunotherapy may be considered in individuals with confirmed allergic sensitization and persistent symptoms despite standard pharmacological treatment.
Despite advances in medical therapy, many patients continue to experience significant nasal obstruction. Long standing hypertrophy characterized by structural changes within the turbinate tissue often demonstrates limited responsiveness to pharmacological interventions. In these circumstances, prolonged reliance on medical treatment alone may unnecessarily delay definitive management. Surgical intervention should therefore be considered when adequate symptom control cannot be achieved through optimized conservative therapy.
Surgical Treatment Options for Inferior Turbinate Hypertrophy
Modern surgical management aims to enlarge the nasal airway while preserving mucosal function. A variety of techniques have been described, each with specific advantages and limitations. Selection of the most appropriate procedure depends upon the underlying pathology, severity of hypertrophy, associated anatomical abnormalities, and surgeon experience.
Radiofrequency turbinate reduction has become one of the most widely utilized minimally invasive techniques. This procedure induces controlled submucosal tissue coagulation, resulting in progressive tissue volume reduction while preserving the overlying mucosa. Patients generally experience minimal postoperative discomfort and rapid recovery. Radiofrequency treatment is particularly suitable for patients with predominantly mucosal hypertrophy and has demonstrated favorable long term outcomes in numerous clinical studies.
Submucosal resection of the inferior turbinate represents another highly effective surgical option. During this procedure, hypertrophic submucosal tissue and occasionally portions of turbinate bone are selectively removed while maintaining mucosal preservation. This technique provides substantial improvement in nasal airflow and is particularly beneficial in patients with significant structural enlargement. Contemporary powered instrumentation techniques have further enhanced surgical precision and reduced postoperative morbidity.
Microdebrider assisted inferior turbinoplasty has gained popularity because of its ability to achieve significant volume reduction while maintaining mucosal integrity. The microdebrider allows precise removal of submucosal tissue under direct visualization, minimizing unnecessary trauma. Several comparative studies have reported excellent functional outcomes and high patient satisfaction rates following microdebrider assisted surgery.
In selected patients, partial turbinectomy may still be considered; however, excessive tissue resection is generally discouraged in modern rhinologic practice. Overaggressive surgery may disrupt normal nasal physiology and predispose patients to chronic dryness, crusting, paradoxical nasal obstruction, and empty nose syndrome. Consequently, contemporary surgical philosophy emphasizes functional preservation rather than radical tissue removal.
Combined Surgical Procedures
Inferior turbinate hypertrophy frequently coexists with septal deviation. In such cases, isolated turbinate surgery may fail to provide optimal airway improvement. Simultaneous septoplasty and turbinate reduction often yield superior functional outcomes because both contributing factors are addressed during the same procedure. Combined surgery has been associated with significant improvement in objective airflow measurements, patient reported symptom scores, and overall satisfaction.
Functional nasal surgery may also be performed concurrently with rhinoplasty procedures in carefully selected patients. Comprehensive correction of both aesthetic and functional abnormalities ensures restoration of nasal breathing while achieving desired cosmetic outcomes. Meticulous preoperative evaluation remains essential to identify all anatomical contributors to airway compromise and develop an individualized surgical plan.
Dr Erdal Erkoç and Advanced Turbinate Surgery
Successful management of inferior turbinate hypertrophy requires extensive experience in functional nasal surgery and thorough understanding of nasal physiology. Dr Erdal Erkoç has dedicated many years to the surgical treatment of nasal airway disorders and has successfully treated a large number of patients suffering from chronic nasal obstruction related to turbinate hypertrophy. Through individualized treatment planning and meticulous surgical technique, Dr Erkoç aims to restore optimal nasal breathing while preserving the physiological functions of the nasal mucosa.
Practicing in Istanbul, Dr Erdal Erkoç routinely performs advanced turbinate reduction procedures either as isolated interventions or in combination with septoplasty and functional rhinoplasty. His surgical philosophy prioritizes tissue preservation, functional restoration, and long term patient satisfaction. Patients undergoing treatment frequently report significant improvements in nasal breathing, sleep quality, daytime energy levels, and overall quality of life following surgery. Such outcomes highlight the importance of expert surgical management in patients whose symptoms remain refractory to medical therapy.
Conclusion
Inferior turbinate hypertrophy represents a highly prevalent and clinically significant cause of chronic nasal obstruction. The condition may profoundly impair sleep quality, daytime functioning, and overall quality of life. Although medical therapy remains the initial treatment modality, many patients ultimately require surgical intervention to achieve durable symptom relief. Modern mucosa preserving surgical techniques provide excellent functional outcomes while minimizing postoperative complications. Early diagnosis, comprehensive evaluation, and individualized treatment strategies remain fundamental principles for successful long term management of this common yet frequently underestimated disorder.




{kind=link}
{kind=link}
{kind=link}